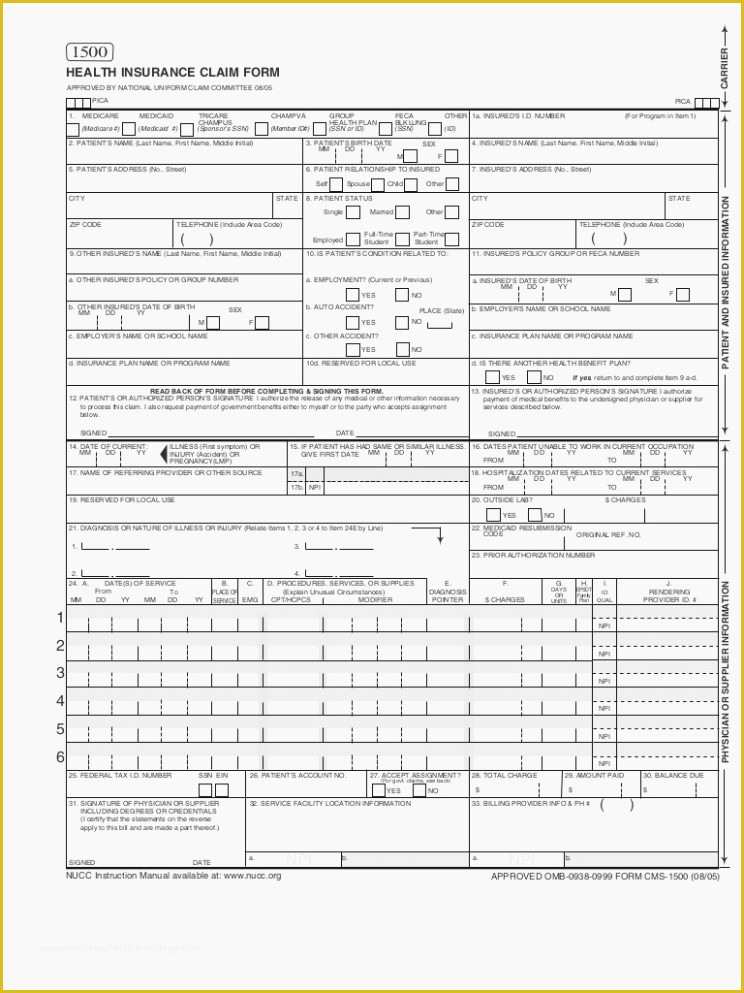
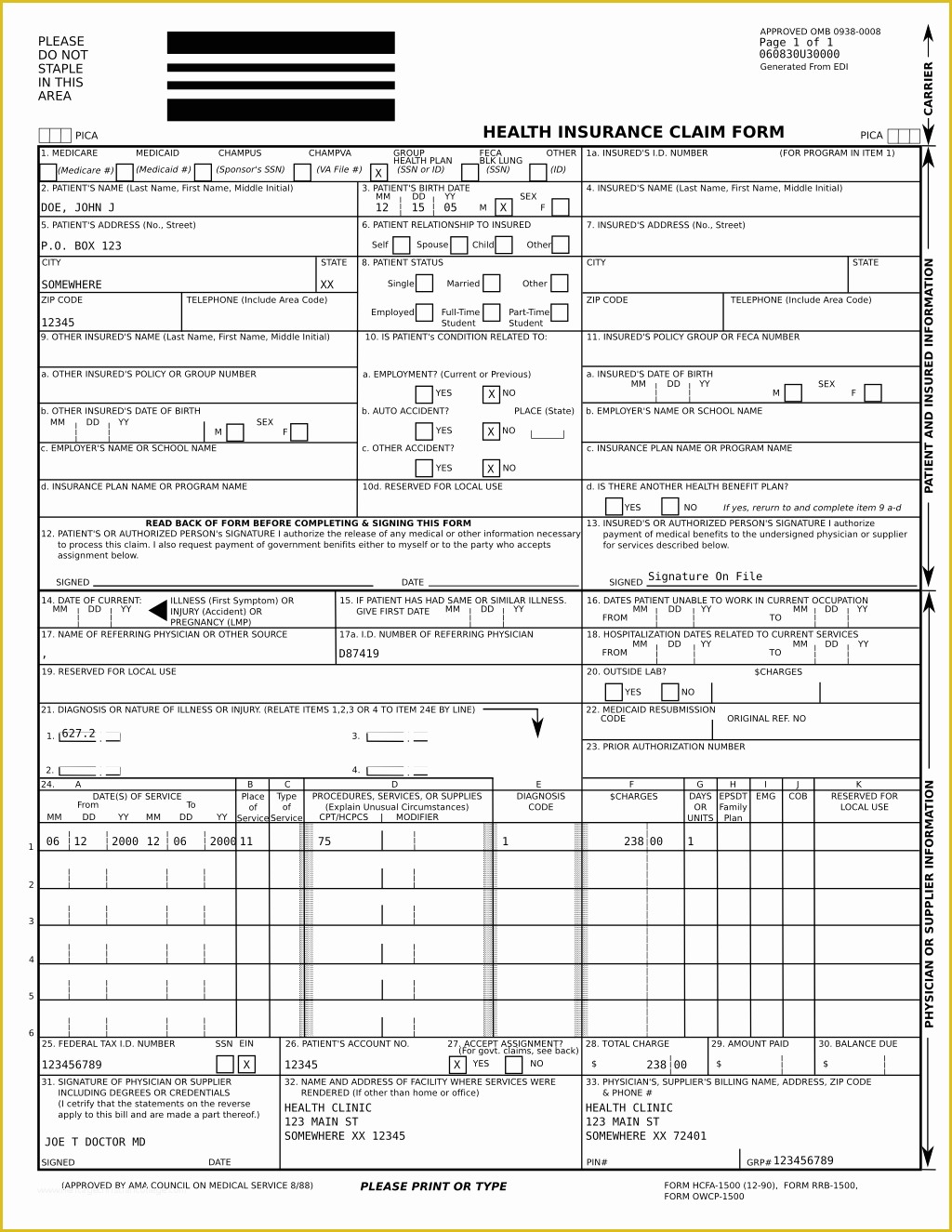
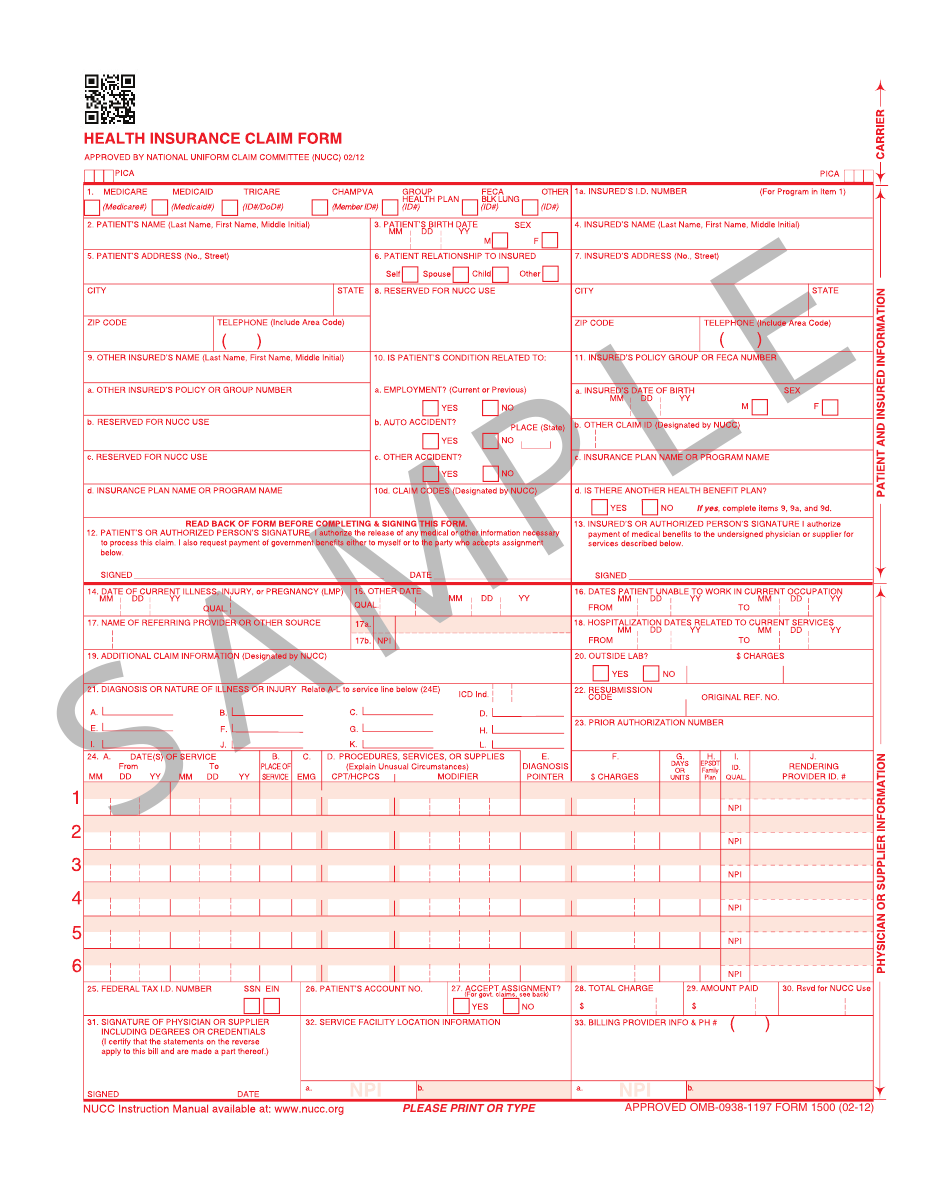
1500 Claim Form Template
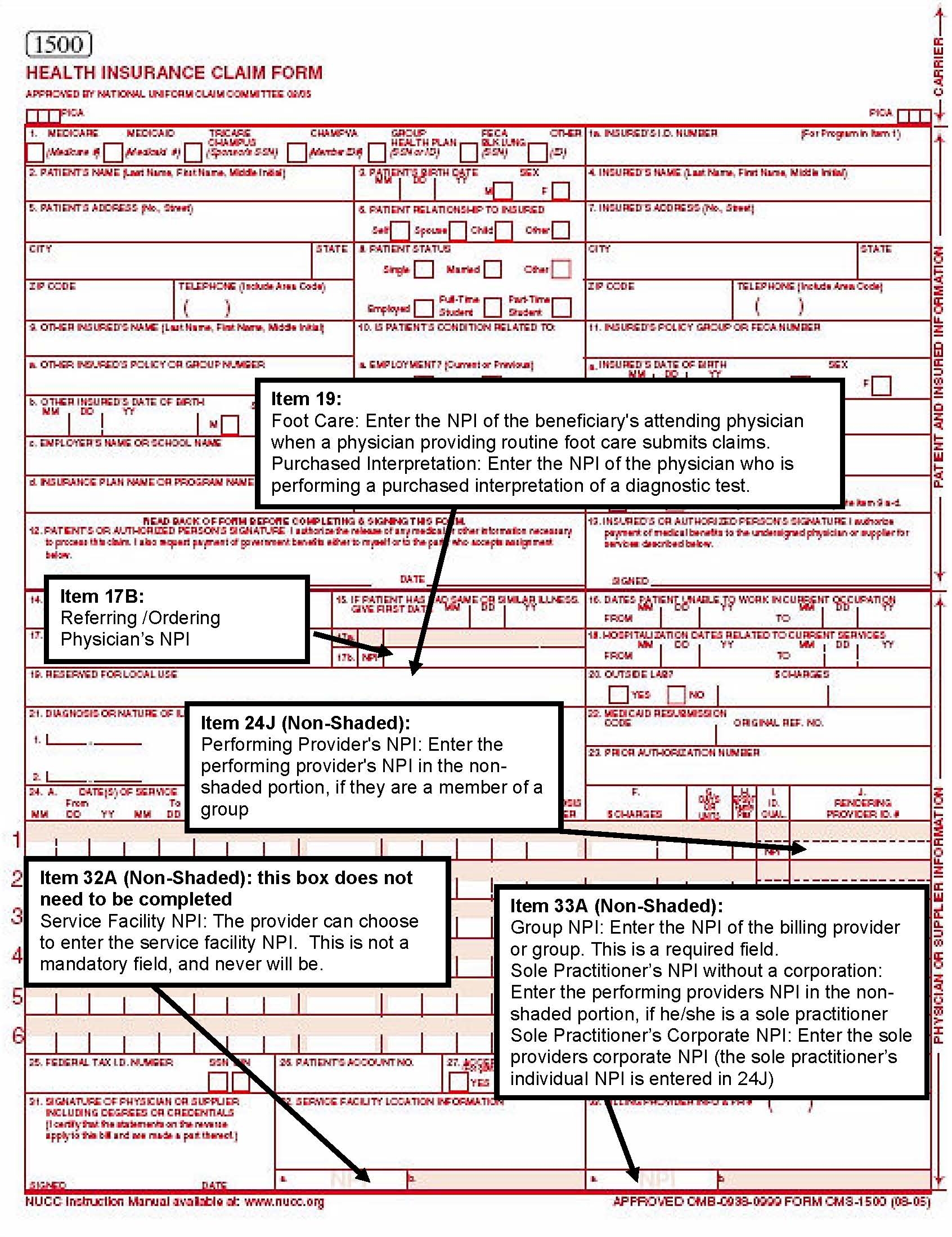
1500 Claim Form Template - You can decide how often to receive updates. You'll see instructions on how to complete the field. Because this form is used by various government and private health programs, see separate instructions issued by applicable programs. Claims may be electronically submitted to a medicare carrier, durable medical equipment medicare administrative contractor (dmemac), or a/b mac from a provider's office using a computer with software that meets electronic filing requirements as established by the hipaa claim. Enter name of the patient. The layout that you see your new claim form in is for editing purposes. (medicare #) (medicaid #) (sponsor’s ssn) patient’s name (last name, first name, middle initial) champva. After being created, you can review the claims from your claims tab. This image of the form should not be used for claims submission. This interactive guide provides instruction on how to complete the orm. This form is the only version accepted by medicare. This is the only format that is accepted. We allow physicians, practitioners, and suppliers to submit a 1500 health insurance claim form under certain situations. The layout that you see your new claim form in is for editing purposes. Web please print or type. You'll see instructions on how to complete the field. Web please print or type. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Read the instructions and tips below first. Our cms 1500 form pdf downloadable is simple to use and comes as a blank cms 1500 claim. Our cms 1500 form pdf downloadable is simple to use and comes as a blank cms 1500 claim form pdf. Approved by national uniform claim committee. Approved by national uniform claim committee (nucc) 02/12. Download free cms 1500 claim form fillable template. We allow physicians, practitioners, and suppliers to submit a 1500 health insurance claim form under certain situations. Do not email completed 1500 claim forms to the nucc. Medicare medicaid tricare champva group health feca blk other. Enter name of the patient. (medicare#) (medicaid#) (id#/do d#) patient’s name (last name, first name, middle initial) champva pica. Box 211256 eagan, mn 55121. Web click create > create claims. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. This image of the form should not be used for claims submission. The layout that you see your new claim form in is for editing purposes. This interactive guide provides instruction on how to complete. Download form 1500 health insurance claim form. Web the 1500 health insurance claim form (1500 claim form) answers the needs of many health care payers. Enter the valid date of birth. Approved by national uniform claim committee. Once printed, your claim form will appear like a normal cms 1500 form. Once printed, your claim form will appear like a normal cms 1500 form. Medicare medicaid tricare champva group health feca blk other. We allow physicians, practitioners, and suppliers to submit a 1500 health insurance claim form under certain situations. This interactive guide provides instruction on how to complete the orm. For more details, see creating batch claims. Group health plan (ssn or id) feca blk lung (ssn). The layout that you see your new claim form in is for editing purposes. Box 211256 eagan, mn 55121. Approved by national uniform claim committee (nucc) 02/12. Failure to follow these guidelines could cause a delay in processing, denial of the claim, or affect payment accuracy. Submit all paper claims to: Please do not staple in this area. Box 211256 eagan, mn 55121. Download form 1500 health insurance claim form. Web health insurance claim form. Web the following is the pdf of the revised 1500 form, including the template and grid versions: Once printed, your claim form will appear like a normal cms 1500 form. The supplier is ultimately responsible for the accuracy of claims filed for his/her services. Download free cms 1500 claim form fillable template. Any person who knowingly files a statement of. Approved by national uniform claim committee (nucc) 02/12. The current version of the original manual from the national uniform claim comettee of how to complete the cms1500 claim form. Sign up to get the latest information about your choice of cms topics. Once printed, your claim form will appear like a normal cms 1500 form. You can decide how often to receive updates. Enter the valid date of birth. It can be purchased in any version required by calling the u.s. Any person who knowingly files a statement of claim containing any misrepresentation or any false, incomplete or misleading information may. The cms claim form is available in red ink. Please do not staple in this area. Medicare ffs contractors include a/b medicare administrative contractors (macs) and durable medical equipment (dme) macs. Web health insurance claim form. Enter name of the patient. This form is the only version accepted by medicare. (medicare #) (medicaid #) (sponsor’s ssn) patient’s name (last name, first name, middle initial) champva. This interactive guide provides instruction on how to complete the orm.
Free Printable Cms 1500 Claim Form
Cms 1500 Claim Form Fillable Free Printable Forms Free Online
Medical Claim Form 1500 templates free printable
Free Fillable Cms 1500 Template
:max_bytes(150000):strip_icc()/CMS-1500-claim-form-57a2d3a85f9b589aa99caf8b.jpg)
Cms 1500 Claim Form Printable
Free Blank Cms 1500 Claim Form Form Resume Examples J3DWAlxOLp
1500 Claim Form PDF Fillable
Form 1500 Fill Out, Sign Online and Download Printable PDF

Completed Cms 1500 Claim Form Sample Form Resume Examples xJKEEg2Krk

Free Cms 1500 Claim Form Template BestTemplates234
Download Free Cms 1500 Claim Form Fillable Template.
Include Any Suffix (Jr., Sr.).
(Medicare#) (Medicaid#) (Id#/Dod#) (Member Id#) Plan (Id#) Lung (Id#) (Id#) 1A.
Failure To Follow These Guidelines Could Cause A Delay In Processing, Denial Of The Claim, Or Affect Payment Accuracy.
Related Post: