Cobra Letter Template
Cobra Letter Template - Find out if you qualify, how to enroll, and what to expect from cobra coverage. Web notice to employees of coverage options. Web the department of labor has developed a model consolidated omnibus budget reconciliation act of 1985 (cobra) continuation coverage election notice that the plan. Web cobra & continuation election notice. Web download the u.s. Web pk !÷> c» : Web this notice contains important information about the right of the enrollee (employee) and qualified dependents (including the enrollee’s spouse and dependent children who are. I just started a new job that provides group health insurance, so i am no longer eligible for the cobra subsidy. Department of labor may be used by group health plans with 20 or more employees to. Web the consolidated omnibus budget reconciliation act (cobra) gives workers and their families who lose their health benefits the right to choose to continue group health. Employers must ensure that a cobra general notice is provided to all eligible group health care participants within 90 days of becoming. How do i notify my former employer that i should no longer. Web download the u.s. Web an example letter to a cobra participant terminating coverage due to selected reason. Department of labor (dol) cobra model election notice. Web notice to employees of coverage options. Web an example letter to a cobra participant terminating coverage due to selected reason. The letter should be sent when an employee is hired and contains special. Department of labor (dol) released a new final rule that. Web this notice contains important information about the right of the enrollee (employee) and qualified dependents. Find out if you qualify, how to enroll, and what to expect from cobra coverage. [enter date of notice] dear: How do i notify my former employer that i should no longer. Cobra election notice (english) this model notice from the u.s. Web notice to employees of coverage options. Web download a free customizable form of the letter that explains employees' rights under cobra law. Web cobra & continuation election notice. Web pk !÷> c» : I just started a new job that provides group health insurance, so i am no longer eligible for the cobra subsidy. [identify the qualified beneficiary(ies), by name or status] this notice contains the. [enter date of notice] dear: Web download a free customizable form of the letter that explains employees' rights under cobra law. Department of labor (dol) cobra model election notice under the regulations section of the dol's cobra continuation coverage webpage. Web the consolidated omnibus budget reconciliation act (cobra) gives workers and their families who lose their health benefits the right. Web dear [employee’s name], as you’re aware, your employment with our company will be ending soon. [enter date of notice] dear: Google docs for freeoffice templates for freeword templates for free Web this notice has important information about your right to continue your healthcare coverage with your group health plan(s), as well as other health coverage options that may be.. Department of labor (dol) released a new final rule that. Google docs for freeoffice templates for freeword templates for free However, our door remains open to you when it comes to. The letter should be sent when an employee is hired and contains special. Web download a free customizable form of the letter that explains employees' rights under cobra law. [enter date of notice] dear: Web download a free customizable form of the letter that explains employees' rights under cobra law. How do i notify my former employer that i should no longer. Web this notice has important information about your right to continue your healthcare coverage with your group health plan(s), as well as other health coverage options that. Web download the u.s. Department of labor (dol) released a new final rule that. Web download a free sample letter to inform employees of their rights and obligations under cobra, the federal law that allows continuation of group health coverage in certain. Web dear [employee’s name], as you’re aware, your employment with our company will be ending soon. Web an. Employers must ensure that a cobra general notice is provided to all eligible group health care participants within 90 days of becoming. I just started a new job that provides group health insurance, so i am no longer eligible for the cobra subsidy. Web download a free customizable form of the letter that explains employees' rights under cobra law. Web. Web the department of labor (dol) on may 2, 2014, released a new model general notice form and model election notice form for providing cobra notices to. Web notice to employees of coverage options. Web download a free sample letter to inform employees of their rights and obligations under cobra, the federal law that allows continuation of group health coverage in certain. How do i notify my former employer that i should no longer. Web the consolidated omnibus budget reconciliation act (cobra) gives workers and their families who lose their health benefits the right to choose to continue group health. Department of labor (dol) cobra model election notice under the regulations section of the dol's cobra continuation coverage webpage. Department of labor may be used by group health plans with 20 or more employees to. Web this notice contains important information about the right of the enrollee (employee) and qualified dependents (including the enrollee’s spouse and dependent children who are. Web this notice has important information about your right to continue your healthcare coverage with your group health plan(s), as well as other health coverage options that may be. Department of labor (dol) released a new final rule that. [identify the qualified beneficiary(ies), by name or status] this notice contains the continuation. Employers must ensure that a cobra general notice is provided to all eligible group health care participants within 90 days of becoming. Web dear [employee’s name], as you’re aware, your employment with our company will be ending soon. Web cobra & continuation election notice. Cobra election notice (english) this model notice from the u.s. Google docs for freeoffice templates for freeword templates for free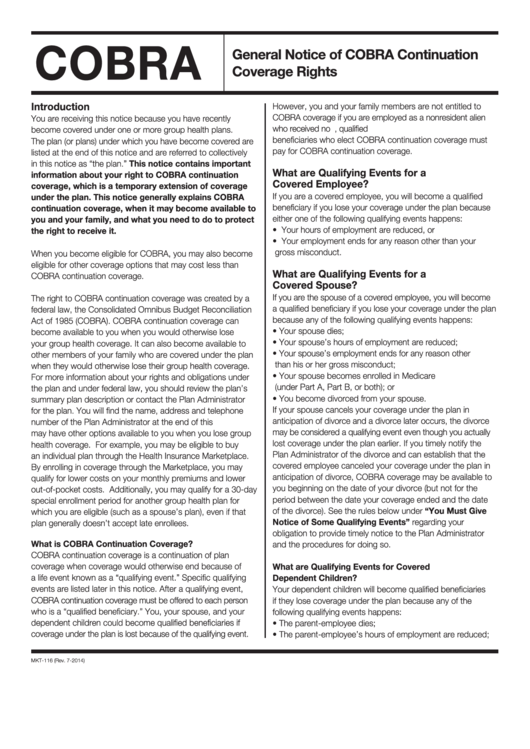
Bcbs General Notice Of Cobra Continuation Coverage Rights Instruction
Cobra Notice Letter Template
Cobra Letter Template Examples Letter Template Collection
Cobra Letter Sample Form Fill Out and Sign Printable PDF Template
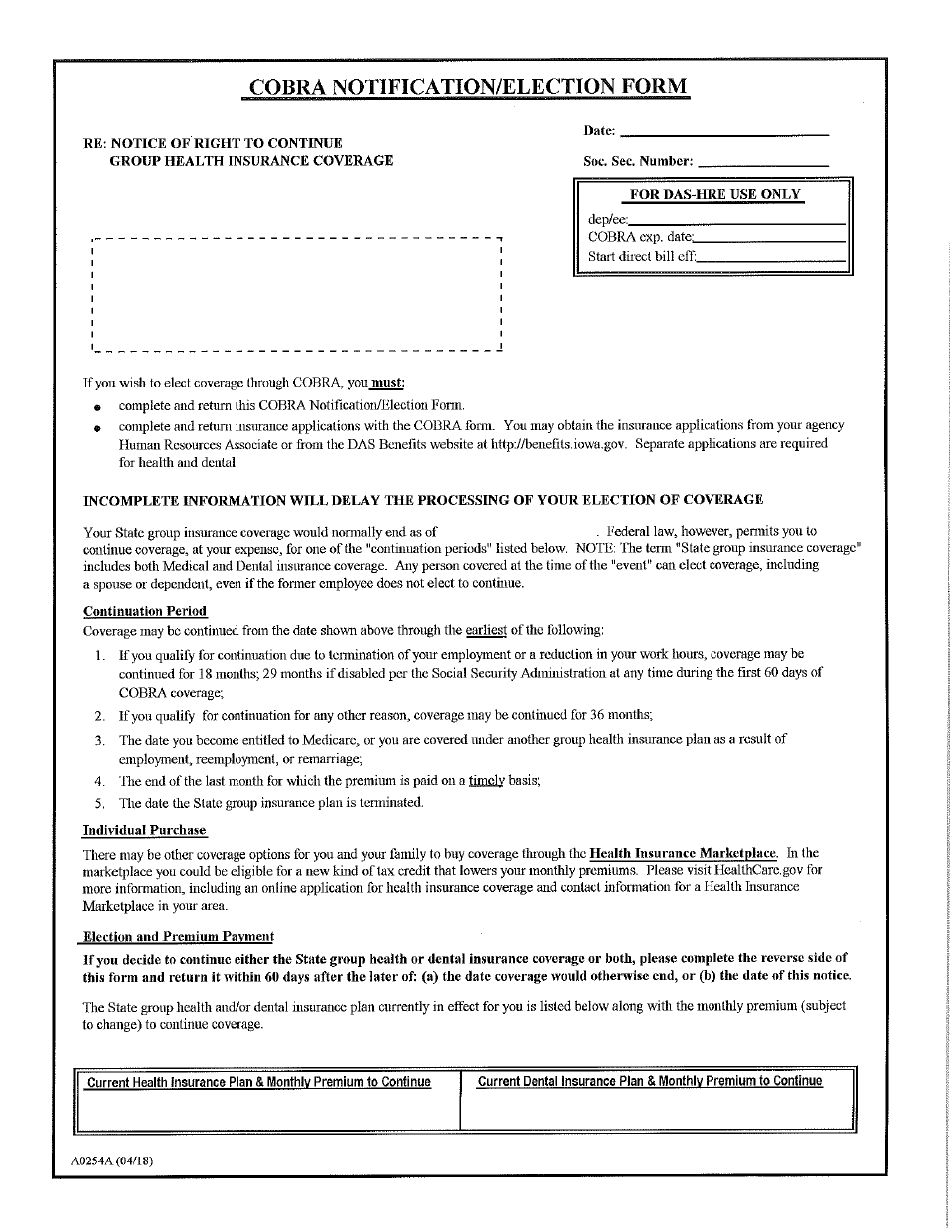
Montgomery Maryland Model COBRA Continuation Coverage Election Notice
Cobra Form Fill Out and Sign Printable PDF Template airSlate SignNow

Sample of Cobra Termination Letter in Word Format Sample Templates

Requesting Cobra Letter for Qualifying Event Fill Online, Printable

COBRA How To Log Into Your Member Portal And Make Your Election

Sample Cobra Letter to Employee 20052024 Form Fill Out and Sign
Web The Department Of Labor Has Developed A Model Consolidated Omnibus Budget Reconciliation Act Of 1985 (Cobra) Continuation Coverage Election Notice That The Plan.
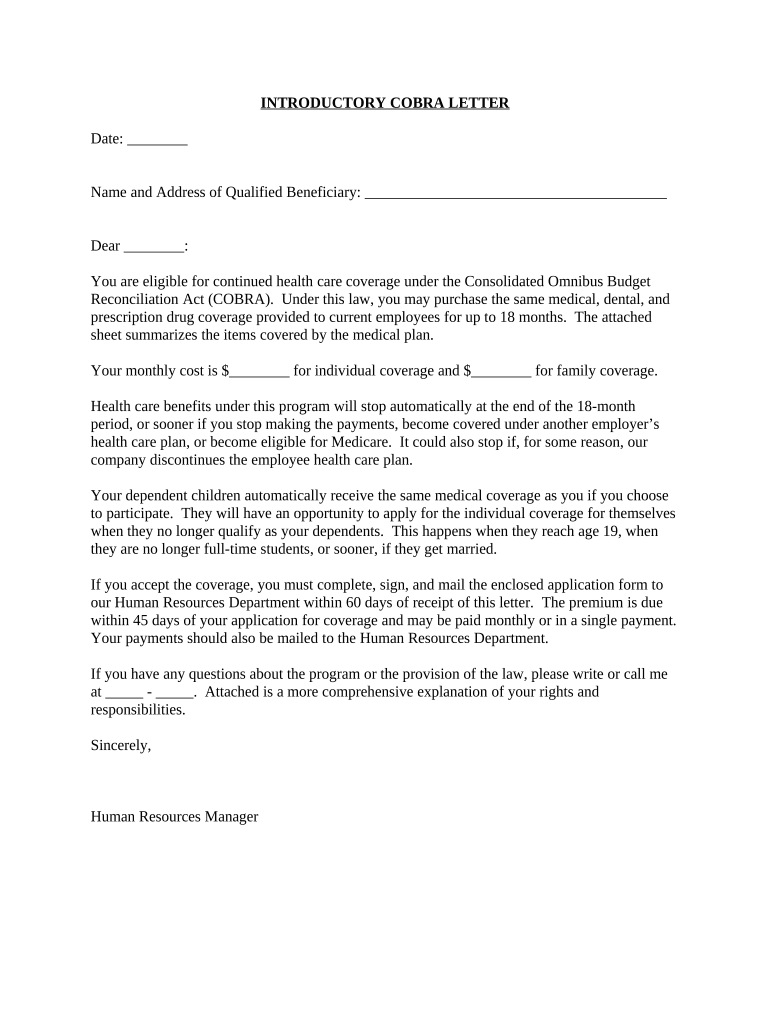
Web Download A Free Customizable Form Of The Letter That Explains Employees' Rights Under Cobra Law.
Web An Example Letter To A Cobra Participant Terminating Coverage Due To Selected Reason.
Page 7 Only To Be Completed By The Plan Administrator And.
Related Post: