Medical Record Request Form Template
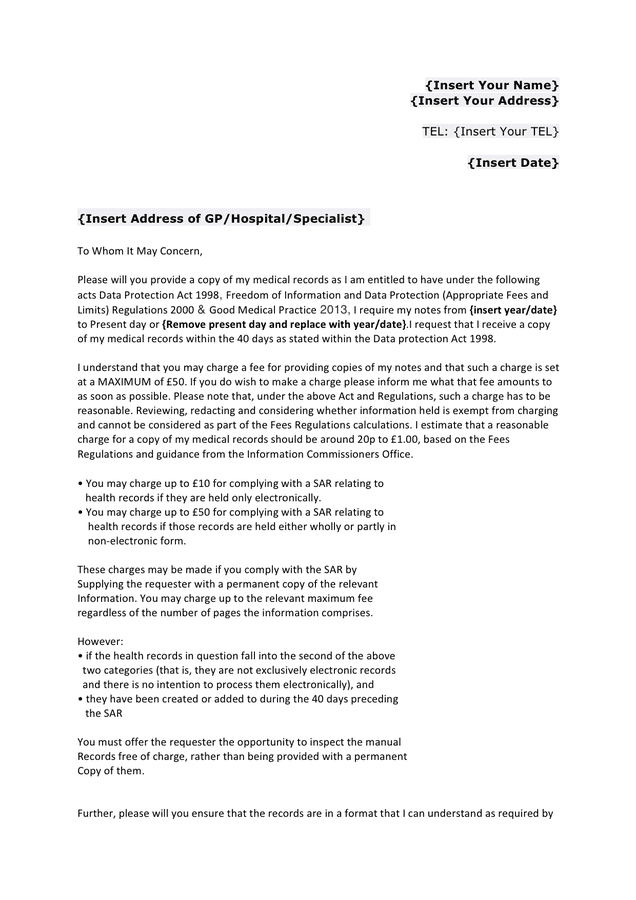
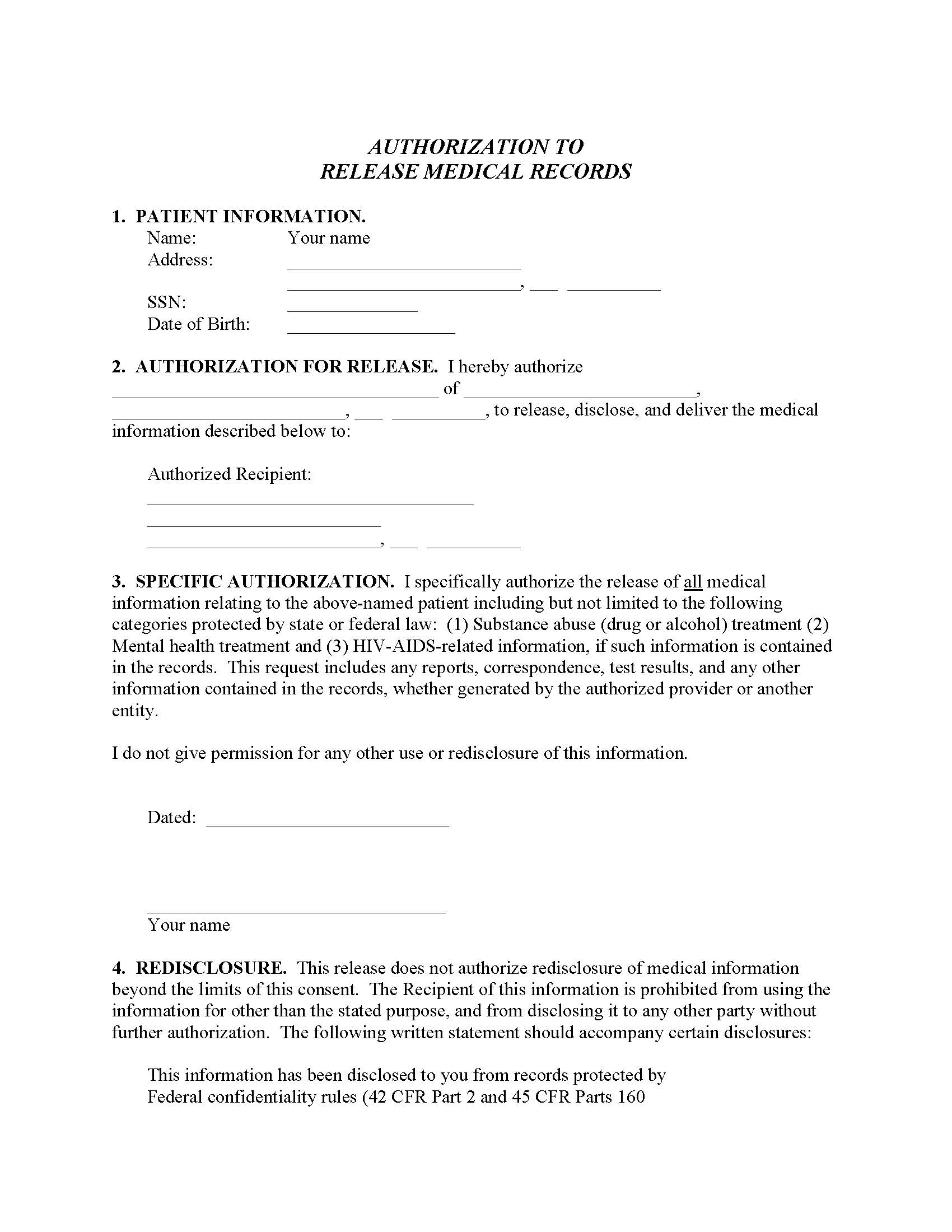
Medical Record Request Form Template - The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health providers not disclose a patient’s information without valid. Powers granted under a medical release can be revoked or reassigned at any time. (name of patient) patient information: Keep patients and other relevant parties in the loop with automated email notifications. It typically includes sections for personal details, medical history, treatment plans, progress notes, and other relevant information. The form user will provide. Web a medical records release (hipaa) form is a written authorization for health providers to release information to the patient and someone other than the patient. Patients generally have the right to their own medical. The second medical release form involves granting permission to administer medical care to a dependent if they. The first form is a medical history release form. Keep patients and other relevant parties in the loop with automated email notifications. You are trying to see a specialist. Free immediate download of pdf. Web the authorization to release protected health information to a third party form is used to authorize the release of health information for insurance, employment, legal or corporate health purposes. Web a medical record template. I may revoke this authorization by sending a written request to the appropriate healthpartners release of information department (see section 8 on back of form). A patient can also request their medical records not currently in their possession. You are in the process of switching doctors. These requests may take up to two weeks to complete. This authorization will be. Log in to myuclahealth portal and fill out the online form. To allow the authorized party to sell my medical records. [your medical identification number or other identifier used] dear. [date] dear [doctor’s name or health records office], i am writing to request a copy of my medical records. You are in the process of switching doctors. I was treated in your office [at your facility] between [fill in dates]. Medical records contain sensitive and personal information and are considered protected and confidential. This authorization will be valid for 1 year from the date of my signature, unless a date, event or condition is otherwise specified. It also allows the added option for healthcare providers to share. It also allows the added option for healthcare providers to share information. Medical records can be sent to another facility with the patient's written consent. Using jotform’s drag and drop builder, you can include your practice’s branding, add or change form fields and checklist. A patient can also request their medical records not currently in their possession. I may revoke. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my health record. You are in the process of switching doctors. Web once signed, a finalized pdf document will be automatically sent to your inbox — ready to download, print, and share for your records. Part 160 and. A patient can also request their medical records not currently in their possession. To allow the authorized party to sell my medical records. You have moved and need to see a new doctor. You have a new insurance policy. Using jotform’s drag and drop builder, you can include your practice’s branding, add or change form fields and checklist. The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health providers not disclose a patient’s information without valid. Log in to myuclahealth portal and fill out the online form. Medical records can be sent to another facility with the patient's written consent. It's used by patients to transfer records from another healthcare facility. You have moved and need to see a new doctor. Medical records contain sensitive and personal information and are considered protected and confidential. Log in to myuclahealth portal and fill out the online form. To allow the authorized party to communicate with me for marketing purposes when they receive payment from a third party. You are trying to see a. Keep patients and other relevant parties in the loop with automated email notifications. For burials & emergency requests. Web a medical records release authorization form is a document that allows a person to disclose protected health information to a third party. The second medical release form involves granting permission to administer medical care to a dependent if they. A patient. These requests may take up to two weeks to complete. Web to request release of medical information please complete and sign this form i, _____hereby voluntarily authorize the disclosure of information from my health record. A patient can also request their medical records not currently in their possession. Web medical release forms are used to request that a healthcare provider share a patient’s medical history with a third party (employer, insurance company, school, etc.). Web components of a medical records request form. Web sending medical records to another facility. You have moved and need to see a new doctor. You manage a medical office and need a new patient's records to put into their chart. I am requesting my medical records for reasons related to my health insurance. The purpose of this letter is to request copies of my medical records as allowed by the health insurance portability and accountability act (hipaa) and department of health and human services regulations. Other medical forms include medical invoices, which both bill and reimburse individuals for health services they may have received, as well as medical. The federal health insurance portability and accountability act of 1996 (hipaa) and state laws mandate that health providers not disclose a patient’s information without valid. Using jotform’s drag and drop builder, you can include your practice’s branding, add or change form fields and checklist. You are trying to see a specialist. Web a medical records release authorization form is a document that allows a person to disclose protected health information to a third party. The medical records request form is a meticulously designed document that serves as the anchor for the secure and efficient exchange of patient information between healthcare providers, patients, and other necessary parties, such as other doctors involved in the patient's treatment.
Medical Record Request Form printable pdf download
Medical Records Request Form in Word and Pdf formats

FREE 12+ Medical Records Request Forms in PDF Word
Medical Records Request Form Template for Health Care Office Etsy
Sample Medical Records Request Form Mous Syusa
Medical Records Request Form download free documents for PDF, Word
Medical Records Request Form download free documents for PDF, Word
Medical Records Request Form download free documents for PDF, Word
Medical Records Request Form Template Free Printable Templates

Printable Medical Record Request Form Template Printable Templates
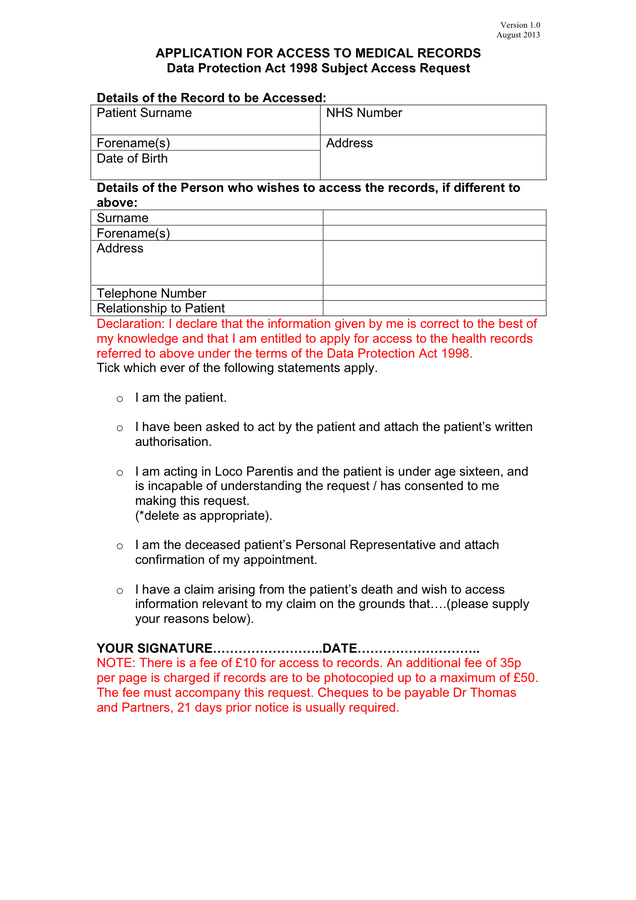
Web Important Names, Addresses, Dates And Signatures.
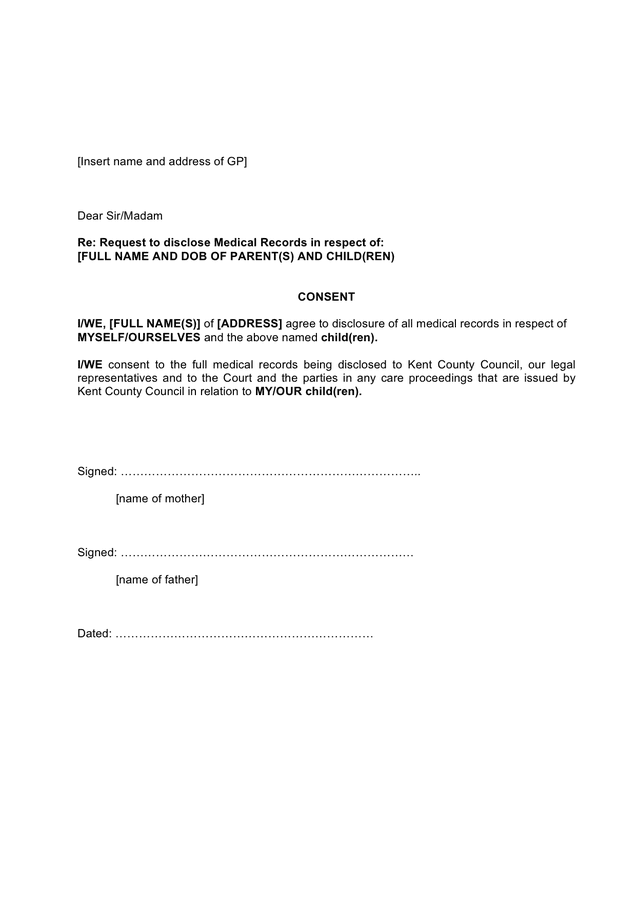
Then, This Form Template Requires The Information For Releasing The Patient’s Medical Records.
I Was Treated In Your Office [At Your Facility] Between [Fill In Dates].
The Form User Will Provide.
Related Post: