Release Of Information Form Template Mental Health
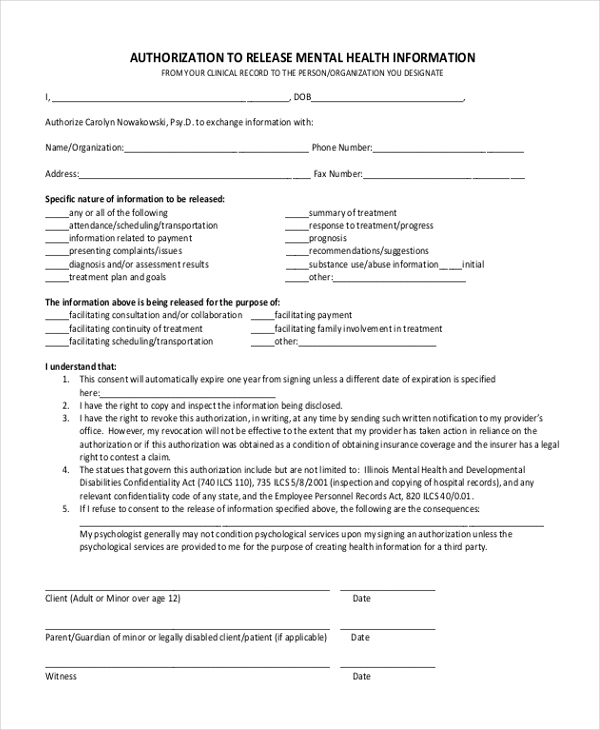
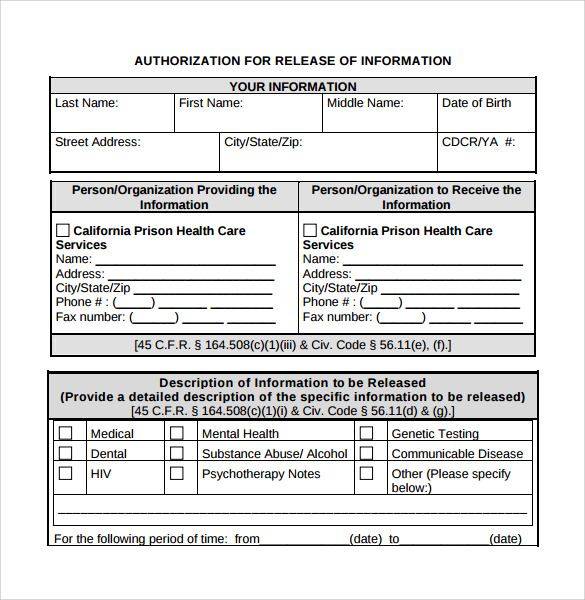
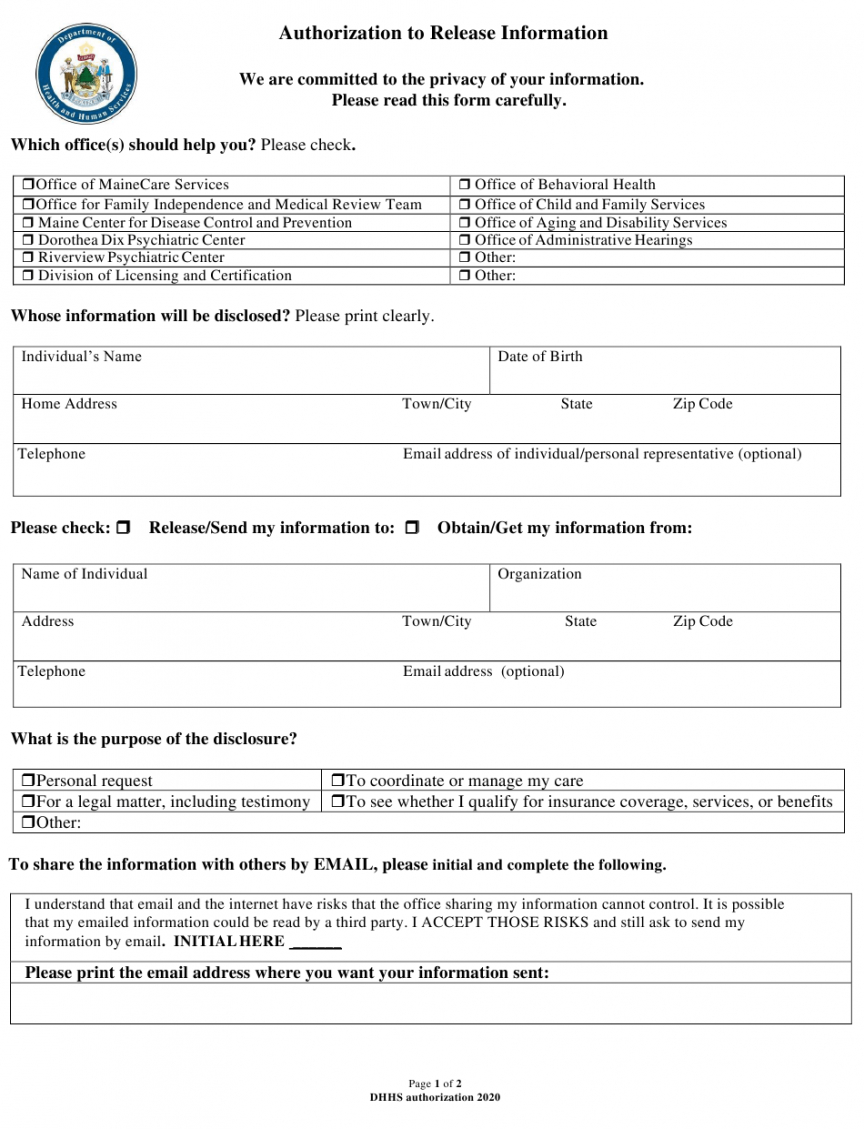
Release Of Information Form Template Mental Health - I authorize ellie mental health 1370 mendota hts rd mendota hts, mn 55120 phone: Web please address questions about this form to the health information management (him) department: Web authorize [insert name of mental health counseling organization] to disclose to and/or obtain from: Hipaa privacy rule cfr section 164.508. Release any mental health or developmental disabilities information or to revoke any previous authorizations, regardless of the _____ patient date of birth: Previous treating therapist, current health care providers, parents or school) client name(s): Web we affirm that the principal is personally known to us, that the principal signed or acknowledged the principal’s signature on this declaration for mental health treatment in our presence, that the principal appears to be of sound mind and not under duress, fraud or undue influence, that neither of us is: Web departmentof health care services. This form, when properly completed, permits the release of confidential information about a person receiving services (service recipient) governed and regulated by title 33, tennessee code annotated. I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that apply)with the following date parameters: _____ patient date of birth: For the rest of your necessary intake forms, check out our easy intake packet, which includes the 7 essential. Web printable mental health release of information form. For the rest of your necessary intake forms, check out our easy intake packet, which includes the 7 essential counseling intake forms you need — all in one instantly downloadable microsoft word template. This template can be used to coordinate the release of confidential information during a client's transition of care or. Authorization for release of information. Authorization for the use and disclosure of protected health information (phi) is only for the person or agency on this form. Any information to be released under this form shall be. ☐assessment ☐care plan ☐individual therapy notes ☐med notes Web authorization to release confidential information. For the purposes of c] treatment/continuing care billing or insurance claims legal proceedings other: Physical and mental health history; Web authorization to release confidential information. For the rest of your necessary intake forms, check out our easy intake packet, which includes the 7 essential counseling intake forms you need — all in one instantly downloadable microsoft word template. I authorize. Web rosecrance’s “authorization to release information” form authorizes rosecrance inc. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. For the purposes of c] treatment/continuing care billing or insurance claims legal proceedings other: And its affiliates (“rosecrance”) to communicate with, release information to, and obtain records and information. Web to release,. Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to disclose/exchange mental health treatment information and records obtained in the course of psychotherapy treatment, including, but not limited to therapist’s diagnosis, of the client listed above to: Web departmentof health care services. Web this authorization is for: Physical and mental health history; Web to release, discuss, or disclose the following: This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. ☐assessment ☐care plan ☐individual therapy notes ☐med notes Authorization for release of information. No responsibility can be accepted if it is made available to any other person or agency. Web to release, discuss, or disclose the following: Form of disclosure unless you have specifically requested in writing that the disclosure be made in a certain format, we reserve the Web the new client intake form can be completed before the first session to capture personal information relating to the client, such as: No responsibility can be accepted if it is made available to any other person or. Form of disclosure unless you have specifically requested in writing that the disclosure be made in a certain format, we reserve the Web this authorization is for: I authorize ellie mental health 1370 mendota hts rd mendota hts, mn 55120 phone: Web click here to instantly download the free release of information form. Use this form to obtain the required. Web rosecrance’s “authorization to release information” form authorizes rosecrance inc. Web click here to instantly download the free release of information form. Previous treating therapist, current health care providers, parents or school) client name(s): This authorization includes information about the following (check all that apply): Web i, ________________________________________, hereby authorize therapy changes (hereinafter “provider”) to disclose/exchange mental health treatment information. Web to release, discuss, or disclose the following: Web authorization to release confidential information. Web authorize [insert name of mental health counseling organization] to disclose to and/or obtain from: Hipaa privacy rule cfr section 164.508. Previous treating therapist, current health care providers, parents or school) client name(s): Web the new client intake form can be completed before the first session to capture personal information relating to the client, such as: Web release of information consent form 1. Web click here to instantly download the free release of information form. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be shared. Hiv/aids test results, diagnosis, or treatment. Download these templates for mental health release of information forms to improve your paperless intake process and hipaa compliance. Full treatment record including all health/mental health information [2 full treatment record excluding the following information: Name, age, and contact details; I authorize the release of any and all of the following medical, mental health and/or substance use disorder information, as specified, which may be contained in my records (check all that apply)with the following date parameters: ☐coordination of care ☐legal ☐personal ☐other (must specify) _____ information to be disclosed: Web printable mental health release of information form.
Release of information template Fill out & sign online DocHub
Free Free Medical Records Release Authorization Form Hipaa Mental
FREE 17+ General Release of Information Forms in PDF Ms Word
FREE 9+ Sample Release of Information Forms in MS Word PDF
Mental Health Release of Information Form PDF airSlate SignNow
Free Mental Health Release Of Information Form
Sample Release Of Information Form Mental Health Classles Democracy

Mental Health Release of Information Form (Editable, Fillable
Free Release Of Information Form Mental Health Template Doc

Mental Health Release of Information Form (Editable, Fillable
Web Departmentof Health Care Services.
Web We Affirm That The Principal Is Personally Known To Us, That The Principal Signed Or Acknowledged The Principal’s Signature On This Declaration For Mental Health Treatment In Our Presence, That The Principal Appears To Be Of Sound Mind And Not Under Duress, Fraud Or Undue Influence, That Neither Of Us Is:
Web Mental Health Treatment I, _____[Insert Name Of Patient/Client], Whose Date Of Birth Is _____, Authorize [Insert Name Of Social Work Organization] To Disclose To And/Or Obtain From:
Web The Following Types Of Information Must Be Specifically Authorized.
Related Post: