Release Of Information Template Mental Health
Release Of Information Template Mental Health - Web authorization for release/exchange of information. Web authorization to release confidential information. Download template download example pdf. This template can be used to coordinate the release of confidential. Please note that a signature of a witness who can attest to the identity of an authorized signatory is required to release any. Web mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of social work organization] to disclose to and/or obtain. Web authorization to release information. I authorize ellie mental health 1370 mendota. This form, when properly completed, permits the release of confidential information. Authorization for the use and disclosure of protected health information (phi) is only. Web if you have to release information regarding mental health from any institution, then you will have to use this form. Web the purpose of this disclosure of information is to share treatment information and to coordinate care. Web health care power of attorney, etc.). Edit your release of information form mental health template online. Download template download example pdf. Printable mental health release of information form. Web to release, discuss, or disclose the following: For the rest of your necessary intake forms, check out our easy intake packet , which includes the 7. Please note that a signature of a witness who can attest to the identity of an authorized signatory is required to release any. Web click here. Hipaa release of information form Web if you have to release information regarding mental health from any institution, then you will have to use this form. In the event of a disclosure necessary for emergency notification,. Web authorization for release of information and medical waiver of liability. This form, when properly completed, permits the release of confidential information. I authorize the release of any and all of the following medical, mental health and/or. Web authorization for release of mental health treatment i, _____[insert name of patient/client], whose date of birth is _____, authorize mindful solutions nj, llc to. Web click here to instantly download the free release of information form. For the rest of your necessary intake forms,. In the event of a disclosure necessary for emergency notification,. Web authorization to release confidential information. Web authorization for release of information and medical waiver of liability. Web authorization for release/exchange of information. • the parent or guardian of an. Web health care power of attorney, etc.). Web authorization for release of information and medical waiver of liability. Web for disclosure of mental health treatment information i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of mental health. Patient information patient full name: Printable mental health release of information form. Authorize therapy changes (hereinafter “provider”) to disclose mental health treatment information and. Web if you have to release information regarding mental health from any institution, then you will have to use this form. Web this authorization is for: 5 star ratedform search enginepaperless solutionsfree mobile app Employee counseling can take many forms and may be performed face to face,. Edit your release of information form mental health template online. Web authorization for release of information and medical waiver of liability. Web to release, discuss, or disclose the following: Web the inspection, copying and/or the release of the individual's protected health information. Web physical and mental health history; ☐coordination of care ☐legal ☐personal ☐other (must specify). Web if you have to release information regarding mental health from any institution, then you will have to use this form. Web for disclosure of mental health treatment information i, _____[insert name of patient/client], whose date of birth is _____, authorize [insert name of mental health. This template can be used to. Hipaa release of information form Web authorization to release confidential information. Web aut h o ri z at i o n f o r re l e as e / e xch ang e o f i nf o rm at i o n. Sign docs electronicallyrocket lawyer guaranteemobile & desktop Patient information patient full name: This form, when properly completed, permits the release of confidential information. Web authorization to release confidential information. Hipaa release of information form Web to release, discuss, or disclose the following: Web authorization for release of information and medical waiver of liability. In the event of a disclosure necessary for emergency notification,. Authorize therapy changes (hereinafter “provider”) to disclose mental health treatment information and. • the parent or guardian of an. Web the inspection, copying and/or the release of the individual's protected health information. Males between 18 and 26 years of age should bring a copy of their selective service system registration. Web this authorization is for: Authorization for the use and disclosure of protected health information (phi) is only. This form provides your therapist with written permission to communicate with other individual providers regarding your. • the individual if they are 12 years of age or older. Employee counseling can take many forms and may be performed face to face,. Web the purpose of this disclosure of information is to share treatment information and to coordinate care.
FREE 9+ Sample Release of Information Forms in MS Word PDF
FREE 13+ Sample Release of Information Forms in PDF MS Word

Mental Health Release of Information Form (Editable, Fillable
Mental Health Release of Information Form (Fillable PDF)
Mental Health Release of Information Form PDF airSlate SignNow

Mental Health Release of Information Form (Editable, Fillable

Information Release form Template Inspirational Release Information

Therapist Release Of Information Template Fill Online, Printable

Mental Health Release Of Information Form & Template Free PDF Download
FREE 17+ General Release of Information Forms in PDF Ms Word
I Authorize Ellie Mental Health 1370 Mendota.
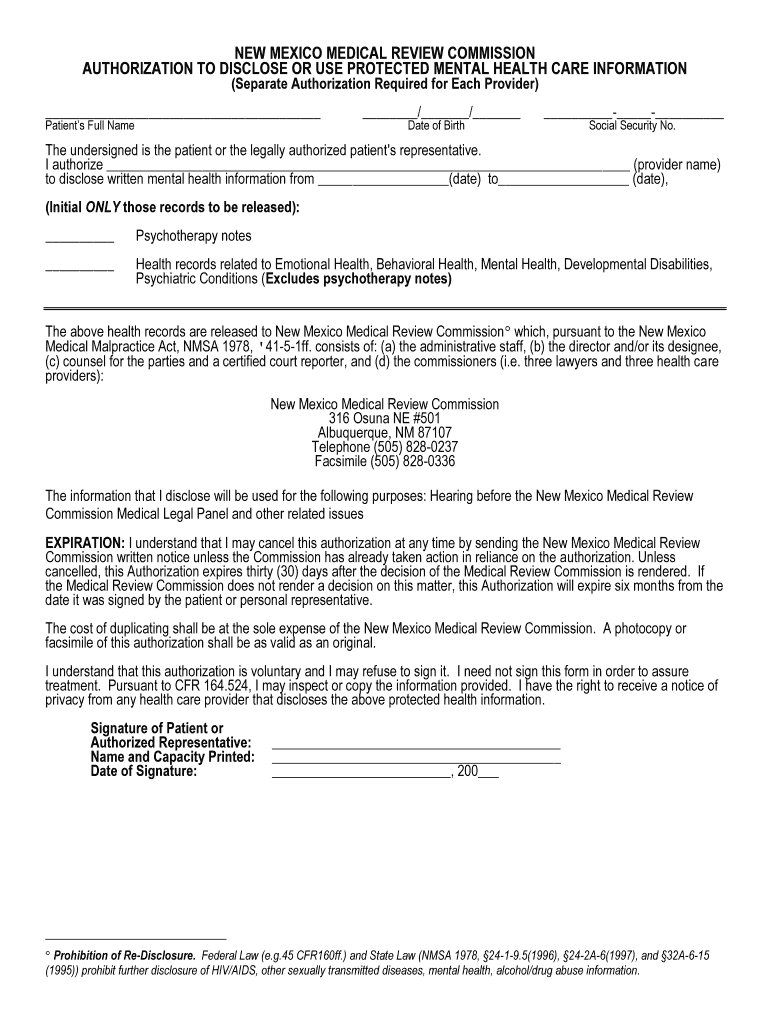
Web If You Have To Release Information Regarding Mental Health From Any Institution, Then You Will Have To Use This Form.
Web The Protected Health Information Indicated Below With:
The Sample Format Is Here.
Related Post: